
Doctor Sapena, 54 6B
03013 – Alicante
674 642 653
Avenida del Mediterraneo 3, bajo
03503 – Benidorm
674 642 653
HLA San Carlos
03700 – Dénia
674 642 653

All breast surgeries, that imply the use of breast implants, generate a capsule around the implant. The capsule is the “internal scar” that the body creates to “isolate” the implant. The capsule is always produced, it is unavoidable. This is a good thing. And it is always like this.
What we see upon operating on a patient who has been a carrier of a breast prosthesis for months or years is always the same. The implant is found with a cover of chalky characteristics.
There are capsules that are very thin, others not so much. There are even some which are very thick which is also completely normal.
Then we have pathological capsules or capsules that make the breast much harder. These, when the surgeon cuts into them, are usually much thicker than the normal ones and can even
fill with a calcium component, which makes them uglier, harder and even as if they have “lumps stuck to them”. It is a capsule that can be clearly seen, which is not normal.
The capsular contracture is what patients describe as: “This breast is harder than the other”. Or even; “This breast is higher than the other and is harder”. And also. “My chest has started to hurt when I lie down”.
The capsular contracture is the hardening of the breast, which is actually the hardening of the capsule that surrounds the implant.
All prosthesis encapsulate. But not all contracture. The reality is, although it is not technically correct, that they are considered exactly the same.
When a patient tells me that they have been told that they have an encapsulated breast, it means that they have been told that it is a contracture.
Correct. Just like many things in life, there are different grades. There are capsular contractures that are very, very mild and others that are very severe. So that the patients have an idea, we are going to divide them into three types. The mild, moderate and severe.
The mild one is usually described by the patients as: “Doctor, in the left breast (for example), I am starting to notice that it is a bit harder than the right. It is not a lot, but I notice one side harder than the other. It doesn’t hurt or bother me. Is this normal doctor?”
The moderate is usually described by patients as: “Doctor, I notice that my left breast (for example) is harder than before. I would even say that although the right one is soft and moves well, the left one is much harder. It also gives me a sensation as if it is moving upwards.
From above I can see that the breast is harder and higher than the other. It does not hurt, but it does not look good with a bra or when wearing blouses”.
This is an established capsular contracture. The affected breast is not only harder than the other, but also, this contracture is making the implant move upwards and causing discomfort to the patient, not only because of the hardness, but also because it has cosmetic implications.
The severe is usually described by the patients like this: “Doctor, I notice my breast much harder than normal. It’s very high. Too high. And also, what worries me the most, is that now it also hurts. It doesn’t just hurt when I lie face down. But also hurts when I receive a hug. It even hurts when I’m watching the television”. This is now a severe capsular contracture.
The severity is not only diagnosed by the more than evident cosmetic consequences, but also because it affects the normal life of the patient. They feel pain. A pain that although it improves with Ibuprofen or Nolotil, is always there. It never disappears completely.
The truth is it cannot. The capsular contracture is something that for now, is always there. What we surgeons have achieved is to reduce it through the measures that we have available to us.
For example. We know that if we insert an implant through the areola, there is more capsular contracture. We know that if we insert the implant on top of the muscle, this also happens. There is also more if the surgeon uses gloves with talc.
And also if the surgeon manipulates the implant with gloves that have not been freshly put on. Smooth prosthesis also enhance the contracture. Not washing the area that we have made for the implant with betadine and/or antibiotics also causes it. Performing sports very soon after the surgery can cause it too.
And even if everything is done well and perfectly, the capsular contracture is there “lurking”.
Classically, the capsular contracture has been treat above all, with what is known as closed capsulotomy. What we used to do was break the capsule using force. The surgeon held the breast and pressed until he heard and felt in his hands a “crack”. This is now completely counter indicated. Primarily because although the effect is immediate and clear, after a short while we find ourselves in the same situation. The capsule starts to “heal” and the breast continues to be contracted. And secondly because it has been related to broken implants.
Medicines for the treatment of asthma have also been used, which seems strange that asthma medicine be used to improve a contracture. And although there are surgeons who say they see improvement, there is no clear evidence of it. Additionally, although there have been some generations of medicine that reduced it, the reality is that they can be harmful to the liver. A clinic where I worked when I finished my residency used it and I can honestly say that I didn’t see any improvement.
If the capsular contracture is mild or moderate, the best thing to do is to leave the patient to evolve. Meaning, do not touch. Always explaining to the patient the situation, what is the evolution and the options they have.
On one hand, if the contracture establishes itself and does not advance, we may not need to operate. If the contracture evolves to severe, surgery with a change of implants and complete capsulotomy is the most common treatment.
Generally and over time, the capsular contractures do not improve on their own and their natural tendency is to get worse.
Is there anything that can improve the contracture and avoid entering the operating theatre?
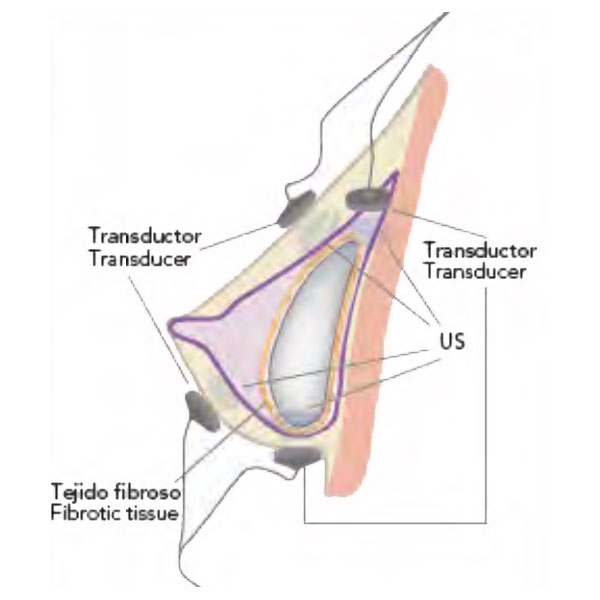
Yes there is. And this is precisely what we offer. Many of these patients, not all, can benefit from the treatment of the capsular contracture through ultrasounds.
With the use of Capsuloblast we can improve, at least one grade, in many of these patients.
We can avoid surgery over a short, medium or long time span. And the treatment can be repeated as many times as needed.
Capsuloblast has been seen as efficient prophylactic treatment for all patients who have breast implants. They do not have a capsular contracture but they want to do their best to avoid one. Lymphatic drains clearly do not work. They are a waste of time and can even favour the capsular contracture with certain types of implants due to its “texture”.
It is also indicated for those patients with capsular contractures that are mild or moderate as it can be capable of improving a grade in such a way that we can avoid surgery for many of them.
In the patients of the severe grade, although there are studies that say that they can also be improved, we need to be honest and more realistic. It can be improved but not cured. There are patients that respond well and say they have less pain.
In cases of severity we can try to postpone the surgery and at least improve the discomfort, temporarily.

Protocol of sessions for both prophylaxis and for treatment of established encapsulation.
We recommend that all patients who are carriers of breast implants, after surgery carry out the following sessions:
1st session. Two weeks after the surgery
2nd session. Three weeks after the surgery
3rd session. A month after the surgery.
4th session. Three months after the surgery
During these sessions we perform the revision of the surgery even if it has been carried out by another colleague, whenever it is necessary.

The protocol that we have established is three sessions a week for a month.
After the first month, it will be necessary to have two sessions a week for another month.
Total: 20 sessions. (The number of sessions can be less or more depending on the grade of the capsular contracture).
Planas et al. Treatment of periprosthetic capsular contracture. 2005.
Escudero et al. Tissue reaction to breast prosthesis. Periprosthetic capsular contracture. An. Sist. Sanit. Navar. 2005; 28 (Supl 2):41-53
Escudero FJ. Tissue reaction on different types of surfaces and locations of silicone breast implants. Experimental comparative study (doctoral thesis). Pamplona: Universidad de Navarra 1991.
Carter D. Tissue reaction to breast implants. Am J Clin Pathol 1994; 102; 565-566
Pardo FJ. Inflammation. Pathological anatomy. Barcelona: Mosby 1997:177-225.
Planas Jorge, et al. Five years’ experience on ultrasonic treatment of breast contractures. Aesthetic Plastic Surgery. March/April 2002.
Planas Jorge et al. External ultrasonic treatment of capsular contract implants. Aesthetic plastic surgery. 21:395-397, 1997.
Planas Jorge, et al. Prophylactic use of external ultrasound for breast implant capsular contracture. Aesthetic Surgery Journal 2002:22:205-207.
Burkhardt, Br. Capsular contracture: Hard breast, soft data. Clin. Plast. Surg. 15:521, 1988.
Georgiada, Ng. Aesthetic surgery of the breast. Philadelphia: WB Saunders. 1990.
Smahel J, Hurwitz N. Soft tissue response to textured silicone implants in an animal experiment. Plastic Reconstr. Surg. 1993; 92; 474-479.
Lossing C, Hanson HA. Peptide growth factors and myofibroblast in capsules around human breast implants. Plastic Reconstr Surg 1993; 91:1277-1286.
Baker JL, Chandler. Occurrence and activity of myofibroblast in human capsular tissue surrounding mammary implants. Plastic Reconstr Surg 1981; 68:905-912
Coleman DJ, Sharpe DT. The role of the contractile fibroblast in the capsules around tissue expanders and implants. BR J Plast Surg 1979:63:700-707
Gayou. A histological comparison of contracted and non-contracted capsules around silicone breast implants. Plastic reconstructive Surg. 1979; 63:700-707
Baker JL Jr. Genesis and management of the hard augmented breast. Adv Plast Reconstr Surg. 1990; 6; 249-268.
Ersek RA,Burroughs. Interrelationship of capsule thickness and breast hardness confirmed by a new measurement method. Plastic reconst Surg 1991:87:1069-1073
Barnett, SB: ter Haar: GR, Ziskin, MC; Nyborg, WL; Maeda, K; Bang, J. Current status of research on biophysical effects of ultrasound. Ultrasound Med. Biol. 1994;20(3);205-1
Robertson, VJ; Baker, KG. A review of therapeutic ultrasound: effectiveness studies. Phys. Ther. 2001 Jul;81(7);1339-50.
Baker, KG; Robertson, VJ; Duck, FA: A review of therapeutic ultrasound: Biophysical Effects. Phys. Ther. 2001;81:1351-1358.
Dinno, MA; Dyson, M; Young, SR; Mortimer, AJ; Hart, J; Crum, LA. The significance of membrane changes in the safe and effective use of therapeutic and diagnostic ultrasound. Phys. Med. Biol. 1989 Nov; 34 (11); 1543-52.
Doan, N; Reher, P; Meghji, S; Harris, M. In Vitro Effects of Therapeutic Ultrasound on Cell Proliferation, Protein Synthesis, and Cytokine Production by Human Fibroblasts, Osteoblasts and Monocytes. J. Oral Maxillofac. Surg. 57;409-419, 1999.
Johns, LD. Nonthermal Effects of Therapeutic Ultrasound: The Frequency Resonance Hypothesis. Journal of Athletic Training. 2002;37(3):293-299.
Mendes, FH; Viterbo, F; DeLuca, L. The Influence of External Ultrasound on the Histologic Architecture of the Organic Capsule Around Smooth Silicone Implants: Experimental Study in Rats. Aesthetic Plastic. Surgery (2008) 32:442-450.
Del Yerro, JL. The Influence of External Ultrasound on the Histologic Architecture or Organic Capsule Around Smooth Silicone Implants: Experimental Study in Rats. Aesthetic Plastic Surgery (2008) 32:451-452
Harpaz, D; Chen, X; Francis, CW; Marder, VJ; Meltzer, RS. Ultrasound Enhancesment of Thrombolysis and Reperfusion In Vitro. JACC. Vol. 21. Nº 6May 1993; 1507-11.
Matheus, JPC; Oliveira, FB; Gomide, LB; Milani, JGPO; Volpon, JB; Shimano, AC. Effects of therapeutic ultrasound on the mechanical properties of skeletal muscles after contusion. Rev. Bras. Fisioter. 2008; 12(3);241-7.
Akinbo, S; Alyegbusi, A; Duru, F; Noronha, C; Okanlawon, A. The Efficacy Of Intrasound Therapy On the Acute Tendon Injury. The Internet Journal of Orthopedic Surgery. 2009 Volume 13 Number 2.
Hüseyin, D; Solmaz, Y; Mehmet, K; Kadri, Y. Comparison of the effects of laser and ultrasound treatments on experimental wound healing in rats. Journal of Rehabilitation Research & Development. Volume 41 Number 5, September/October 2004. Pages 721-728.
Feril, LB; Kondo, T. Biological Effects of Low Intensity Ultrasound; The Mechanism Involved and its Implications on Therapy and Biosafety of Ultrasound. J. Radiat. Res. Vol. 45, Nº 4 (2004); hhtp://jrr.jsatege.jst.go.jp.
Young, SR; Dyson, M. Macrophage responsiveness to therapeutic ultrasound. Ultrasound Med. Biol. 1990;16(8):809-16.
Freitas, TP; Gomes, M; Fraga, DB; Freitas, LS; Rezin, GT; Santos, PM; Silveira, PC; Paula, MM; Pinho, RA; Streck, EL. Effect of Therapeutic Pulsed Ultrasound on Lipoperoxidation and Fibrogenesis in an Animal Model of Wound Healing. US J. Surg. Res. 2009 May 13.
This website uses cookies so that we can provide you with the best user experience possible. Cookie information is stored in your browser and performs functions such as recognising you when you return to our website and helping our team to understand which sections of the website you find most interesting and useful.
Strictly Necessary Cookie should be enabled at all times so that we can save your preferences for cookie settings.